June 22, 2026
A Biomedical Blind Spot Collides With a Global Resource Crisis
When epidemiologists design vaccine development pipelines, they prioritise pathogens by mortality burden, outbreak frequency, and pandemic potential. That logic is rational, yet it produces a structural vulnerability that becomes visible only when a lower-priority pathogen escapes its historical envelope. The DR Congo Bundibugyo Ebola outbreak of 2026 is precisely that scenario: a strain long considered a secondary threat, consistently overshadowed by its more lethal Zaire cousin, has now surpassed 1,000 confirmed infections and ignited a public health emergency at the geographic heart of the world's most strategically sensitive mineral corridor.
Understanding how this happened, why containment has proven so difficult, and what the cascading economic consequences could look like requires moving beyond case counts and into the underlying systems that allowed a rare filovirus to reach this scale.
When big ASX news breaks, our subscribers know first
The Virology Behind the Vaccine Gap
Six Species, One Dominant Research Focus
The genus Ebolavirus within the family Filoviridae contains six recognised species: Zaire ebolavirus, Sudan ebolavirus, Taï Forest ebolavirus, Reston ebolavirus, Bombali ebolavirus, and Bundibugyo virus (BDBV), as classified by the International Committee on Taxonomy of Viruses and referenced by both the World Health Organization and the U.S. Centers for Disease Control and Prevention. Each carries a distinct antigenic and genetic profile, meaning antibodies and vaccine-induced immune responses generated against one species do not reliably neutralise another.
This taxonomic separation is not a technicality; it is the core reason the DR Congo Bundibugyo Ebola outbreak presents such a formidable containment challenge. Two vaccines are currently licensed for Ebola virus disease, both targeting Zaire ebolavirus: the single-dose rVSV-ZEBOV (Ervebo), approved by both the European Medicines Agency and the U.S. Food and Drug Administration in 2019, and the two-dose Ad26.ZEBOV/MVA-BN-Filo regimen (Zabdeno/Mvabea), approved in the European Union in 2020. Neither has been licensed specifically for Bundibugyo virus, and large-scale efficacy data against BDBV remains absent from the published clinical literature.
The absence of a Bundibugyo-targeted vaccine is not an oversight. It reflects a decade of understandable but consequential prioritisation, shaped by the 2014 to 2016 West Africa epidemic involving Zaire ebolavirus, which killed more than 11,000 people and mobilised the largest international Ebola response in history. That emergency accelerated Zaire-focused countermeasure development at the expense of a balanced cross-species pipeline.
Bundibugyo's Clinical Profile: Lower CFR, No Less Dangerous
Bundibugyo virus was first characterised during an outbreak in Bundibugyo District, western Uganda, in 2007 and 2008, where researchers documented 149 suspected and confirmed cases and 37 deaths, yielding a case fatality ratio of approximately 25 percent in that event (Towner et al., PLoS Pathogens, 2008). Subsequent analyses by WHO and Ugandan health authorities produced case fatality ratio estimates ranging between roughly 25 and 36 percent, depending on case classification methodology and whether deaths outside clinical settings were captured.
Those figures compare favourably to the historical peak CFRs associated with Zaire ebolavirus, which reached up to 90 percent in early outbreaks such as Yambuku in 1976 and Kikwit in 1995, where limited supportive care and delayed recognition compounded virological severity. However, a 25 to 36 percent CFR in health systems lacking intensive care capacity, reliable cold chains, and adequate isolation infrastructure remains catastrophic in absolute terms.
A critical and underappreciated epidemiological feature of Bundibugyo is the challenge it poses to peripheral diagnostics. Strain-specific identification requires laboratory infrastructure that most rural or conflict-adjacent health facilities in eastern DRC simply do not possess. The result is a delay between symptom onset and confirmed diagnosis during which community transmission continues, often invisible to official surveillance systems. Doctors Without Borders has outlined why this Bundibugyo outbreak is distinctly challenging compared to prior Ebola emergencies, reinforcing these diagnostic and operational concerns.
Decoding the Numbers: What 1,000 Cases Actually Represents
Confirmed Data Against a Backdrop of Systematic Under-Ascertainment
The figures below represent confirmed data points from the 2026 DR Congo Bundibugyo Ebola outbreak, drawn from reporting by Business Insider Africa (Ayodeji Adegboyega, 22 June 2026) and cross-referenced against publicly available WHO situation updates:
| Metric | Reported Figure | Reference Point |
|---|---|---|
| Confirmed cases, DRC | 1,003 | Late June 2026 |
| Confirmed deaths, DRC | 254 | Late June 2026 |
| Confirmed cases, DRC (prior) | 837 | 15 June 2026 |
| Confirmed deaths, DRC (prior) | 196 | 15 June 2026 |
| Confirmed cases, Uganda | 19 | Mid-June 2026 |
| Deaths, Uganda | 2 | Mid-June 2026 |
| U.S. CDC emergency funding | $107 million | June 2026 |
The jump from 956 cases to 1,003 within a single 24-hour reporting window is among the most telling data points in the entire dataset. It signals that transmission is accelerating rather than plateauing, a trajectory that conflicts directly with what would be expected if containment measures were gaining traction.
Why the True Infection Count Is Almost Certainly Far Higher
Several structural factors combine to suppress official case counts well below the epidemiological reality:
- Contact tracing saturation: Health authorities have acknowledged that tens of thousands of potential contacts linked to confirmed patients remain untraced, a surveillance gap that grows geometrically as case counts rise.
- Conflict-restricted access: Active operations by multiple armed groups across Ituri, North Kivu, and South Kivu provinces physically prevent response teams from reaching communities where transmission may already be well established.
- IDP camp transmission: In at least one internally displaced persons camp in northeastern DRC, more than 30 deaths were recorded from May 2026 onward, with confirmed Ebola-linked fatalities among them, suggesting community-level spread that runs ahead of formal detection.
- Healthcare-associated transmission: WHO has specifically flagged transmission within clinical settings as a concern, indicating that hospitals and health posts, which should function as containment points, are instead functioning as amplification nodes in areas lacking adequate infection prevention infrastructure.
- Peripheral diagnostic limitations: Without strain-specific point-of-care diagnostics in rural facilities, Bundibugyo cases can be misclassified as other febrile illnesses, meaning they never enter the official count at all.
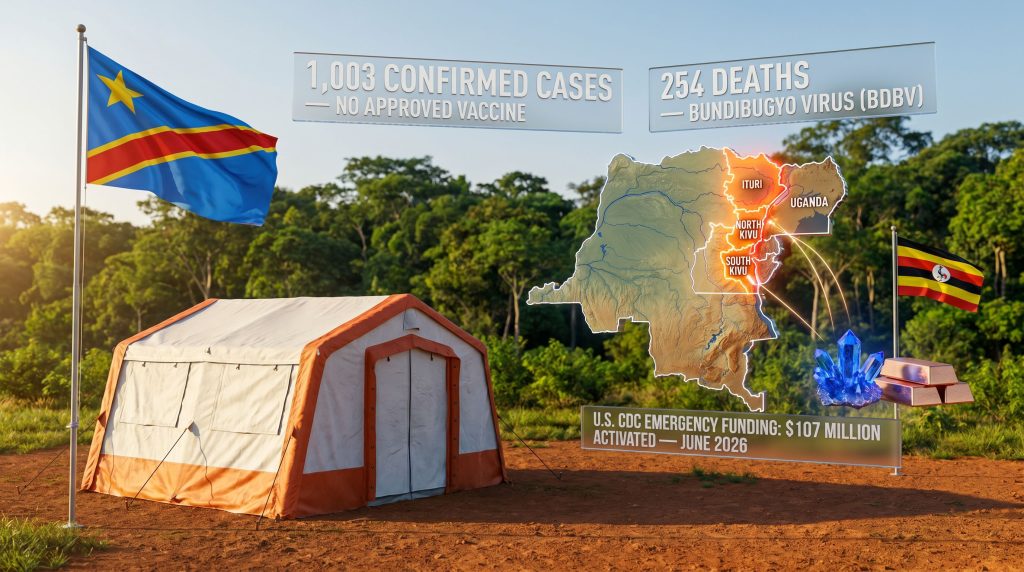
As of late June 2026, the DR Congo Bundibugyo Ebola outbreak has surpassed 1,003 confirmed cases and 254 deaths in DRC alone, with 19 confirmed cases and 2 deaths in Uganda. Health officials warn the true infection count is likely significantly higher due to contact tracing limitations, active conflict, and surveillance gaps across affected provinces.
The Structural Conditions That Enabled This Scale
Decades of Conflict as an Epidemiological Multiplier
Eastern DRC has hosted dozens of armed groups operating across Ituri and the Kivu provinces for the better part of three decades. This is not simply background noise to the outbreak; it is a primary determinant of why containment has failed to contain. The 2018 to 2020 North Kivu Ebola outbreak, caused by Zaire ebolavirus and ultimately the second-largest Ebola outbreak in recorded history, demonstrated with painful clarity how insecurity extends outbreak duration, increases mortality, and forces response teams to operate at reduced capacity in the zones of highest transmission.
Chronic underfunding of health infrastructure across the affected provinces means that the baseline from which response teams are working is extraordinarily low:
- Community health worker networks are under-resourced and under-trained for filovirus response protocols.
- Isolation facilities in peripheral health zones lack the structural integrity to prevent nosocomial spread.
- Cold-chain logistics, essential for any future vaccine deployment, are disrupted across conflict corridors.
- Coordination between national and provincial health authorities is fragmented by insecurity and administrative dysfunction.
Population Mobility and the Cross-Border Transmission Pathway
Eastern DRC occupies a pivotal position within regional migration and trade corridors connecting the country to Uganda, Rwanda, Burundi, and Tanzania. Mining activity, particularly cobalt and copper extraction across Ituri and the Copperbelt-adjacent zones, generates a continuous flow of workers, traders, and support personnel across provincial and international borders. This mobility is economically essential to the region, yet from a virology standpoint it creates transmission chains that respect neither provincial boundaries nor national borders.
WHO has explicitly identified population movement linked to mining operations and cross-border trade as a material risk factor for regional spread. Furthermore, Uganda's confirmed case tally of 19 infections and 2 deaths by mid-June 2026 validates this risk model: the virus reached a neighbouring country through exactly the pathways health officials had flagged as high-risk.
Historical Scale: How This Outbreak Compares
The Largest Ebola Outbreaks in Modern History
| Outbreak | Strain | Total Cases | Deaths | Duration |
|---|---|---|---|---|
| 2014 to 2016 West Africa | Zaire | ~28,600 | ~11,325 | ~2 years |
| 2018 to 2020 North Kivu, DRC | Zaire | ~3,481 | ~2,299 | ~2 years |
| 2022 Uganda | Sudan | ~142 | ~55 | ~4 months |
| 2007 to 2008 Bundibugyo, Uganda | Bundibugyo | ~149 | ~37 | ~4 months |
| 2026 DRC and Uganda (ongoing) | Bundibugyo | 1,003+ | 254+ | Ongoing |
The 2026 event has already eclipsed the total case count of every previous Bundibugyo strain outbreak by a factor of more than six. It is consequently the largest recorded Bundibugyo outbreak in history by a substantial margin, and if the trajectory suggested by the 24-hour reporting spike holds, comparisons to the North Kivu Zaire outbreak become increasingly relevant.
Africa CDC has warned publicly that without rapid containment, this event could rank among the most severe Ebola emergencies in modern history. That framing is significant: Africa CDC typically applies cautious institutional language, making such statements a meaningful signal of how seriously continental health authorities regard the current trajectory.
Understanding the PHEIC Designation
WHO has formally declared the 2026 DR Congo Bundibugyo Ebola outbreak a Public Health Emergency of International Concern (PHEIC) under the International Health Regulations (IHR 2005). This designation sits at the apex of the WHO alert framework and triggers legally binding reporting obligations on member states, accelerated international financing mechanisms, and expedited regulatory pathways for experimental countermeasures.
Internally, WHO's risk classification for DRC is assessed as very high, reflecting three simultaneous conditions: sustained community transmission, confirmed geographic expansion into new health zones, and cross-border spread to Uganda. This classification framework means response teams are operating in the highest-urgency tier of the WHO's escalation architecture.
The International Response and Its Gaps
Emergency Financing and Multilateral Coordination
The scale of international financial mobilisation reflects how seriously external actors regard the outbreak's trajectory:
- The U.S. CDC activated $107 million in emergency funding to support response operations in both DRC and Uganda, one of the largest single emergency health appropriations directed at an African outbreak in recent years.
- Africa CDC has deployed rapid response teams and is coordinating with national health ministries across the Great Lakes region.
- The Afreximbank annual meeting, a flagship African financial summit, was cancelled partly due to concerns over Ebola-related travel and trade disruption, demonstrating the outbreak's reach into institutional and economic decision-making beyond the health sector.
The Experimental Countermeasures Landscape
Without a licensed Bundibugyo vaccine, response architects face a countermeasure void that fundamentally changes the tactical options available. Ring vaccination, which proved highly effective during the 2018 to 2020 North Kivu Zaire outbreak, cannot be deployed in its standard form because it requires a validated vaccine matched to the circulating strain.
Several avenues are under active consideration or likely to be invoked:
- Compassionate use frameworks for experimental Bundibugyo-candidate vaccines that have cleared early-phase clinical evaluation but not full licensure.
- Cross-reactive monoclonal antibody therapies: Treatments such as mAb114 and REGN-EB3, developed and validated against Zaire ebolavirus, may offer partial cross-reactive benefit against Bundibugyo, though efficacy data from large-scale trials against BDBV specifically does not yet exist.
- WHO R&D Blueprint activation: The Blueprint framework, designed to fast-track countermeasure development for priority pathogens, is expected to be used to compress Bundibugyo-specific research timelines.
- Supportive care optimisation: In the absence of targeted therapeutics, aggressive supportive care including fluid and electrolyte management, broad-spectrum antimicrobials, and analgesic protocols remains the primary clinical intervention, and its effectiveness is reflected in the more than 100 confirmed recoveries recorded as of late June 2026.
The core challenge is that ring vaccination was the containment cornerstone in recent Zaire outbreaks. Without a Bundibugyo equivalent, response teams must rely entirely on epidemiological surveillance, aggressive isolation, and community-level behaviour change, tools that are effective but vastly harder to operationalise at scale in conflict-affected terrain.
The next major ASX story will hit our subscribers first
When a Health Crisis Meets a Critical Minerals Corridor
DRC's Irreplaceable Position in Global Supply Chains
The economic dimension of this outbreak is not incidental. DRC accounts for approximately 70 to 75 percent of global cobalt production and ranks among Africa's largest copper producers. The natural resources in the DRC, including both minerals, are foundational inputs for electric vehicle battery cathodes, grid-scale energy storage systems, and a broad range of advanced electronics. The provinces at the epicentre of the outbreak, Ituri, North Kivu, and South Kivu, overlap directly with or sit immediately adjacent to the Congolese Copperbelt and artisanal cobalt extraction zones that feed into global supply chains.
This geographic coincidence elevates the 2026 outbreak to a category distinct from most prior Ebola emergencies. Previous outbreaks in more economically peripheral zones carried tragic human costs without triggering significant global supply chain exposure. The 2026 event carries both simultaneously.
How Outbreak Dynamics Translate Into Commodity and Investment Risk
The mechanisms through which a sustained outbreak in eastern DRC could affect global critical minerals markets operate across several interconnected channels. In addition, the ongoing DRC cobalt export ban has already introduced pre-existing supply constraints, meaning that any further disruption from the outbreak compounds an already pressured market environment.
- Workforce absenteeism and operational disruption: Disease burden in mining communities reduces the labour available for extraction, processing, and transport operations, directly compressing output volumes.
- Movement restriction pressures: Cross-border transmission risk creates political pressure on Uganda, Rwanda, Zambia, and other transit nations to implement travel or trade screening measures that could slow mineral export logistics.
- Foreign direct investment hesitancy: Prolonged outbreak duration historically correlates with reduced investor appetite for resource projects in affected regions, potentially delaying mine development timelines already constrained by infrastructure deficits.
- EV battery supply chain vulnerability: Companies and governments pursuing electric vehicle localisation strategies, particularly in the United States, European Union, and Japan, face heightened cobalt sourcing uncertainty if the outbreak persists through the second half of 2026.
- Artisanal mining sector exposure: A substantial proportion of DRC cobalt output comes from artisanal and small-scale mining operations with minimal occupational health infrastructure and high workforce mobility, making them both epidemiologically vulnerable and operationally fragile under outbreak conditions.
The cobalt price impacts stemming from prior supply disruptions in the region offer a useful precedent for understanding how market participants may respond to a sustained outbreak scenario. Furthermore, given the Congolese cobalt rivalry between major powers competing for influence over DRC's mineral output, any prolonged instability carries geopolitical dimensions that extend well beyond commodity pricing alone.
| Supply Chain Risk Factor | Affected Actors | Potential Impact |
|---|---|---|
| Workforce absenteeism | Mining operators, smelters | Output volume reduction |
| Movement restrictions | Exporters, traders, logistics firms | Shipment delays, cost increases |
| FDI hesitancy | Junior and mid-tier miners | Project financing delays |
| EV battery sourcing uncertainty | Automakers, battery manufacturers | Procurement strategy rethink |
| Artisanal sector disruption | Global cobalt spot market | Price volatility |
Disclaimer: The above represents a risk framework based on historical outbreak patterns and publicly available economic data. It does not constitute investment advice. Commodity market outcomes depend on multiple variables, and investors should seek independent financial guidance.
A Five-Pillar Framework for Containment
What an Effective Response Architecture Requires
Containment at this scale requires simultaneous progress across five interconnected operational pillars:
- Accelerated and expanded contact tracing: Deploying additional trained teams with embedded community liaison support to close the surveillance gap between official case counts and estimated true infection totals. Digital contact tracing tools piloted during prior DRC outbreaks offer a scalable model if connectivity infrastructure permits.
- Negotiated humanitarian access: Establishing and maintaining humanitarian corridors with armed groups operating across affected provinces, allowing response teams to reach high-transmission communities currently inaccessible due to active conflict.
- Compressed experimental vaccine evaluation: Invoking WHO's R&D Blueprint to advance Bundibugyo-specific vaccine candidates through adaptive clinical trial designs with compressed evaluation timelines, prioritising safety and immunogenicity data that could support compassionate use authorisation.
- Regional border health coordination: Implementing standardised screening, notification, and case-management protocols at DRC's borders with Uganda, Rwanda, Burundi, and Tanzania, with particular attention to crossing points associated with mining sector workforce movement.
- Community trust infrastructure: Investing in locally led health communication campaigns that address treatment avoidance, reduce stigma, and improve voluntary case reporting in communities where prior negative experiences with outbreak response operations have eroded institutional trust.
DRC's Track Record and the Limits of Historical Precedent
DRC has successfully contained multiple prior Ebola outbreaks, including several caused by the Zaire strain, demonstrating that institutional knowledge and response capacity exist within the system. However, each of those successful containments benefited from at least one of the following advantages: a geographically bounded outbreak, a licensed vaccine for the circulating strain, or a security environment that permitted meaningful health worker access. The 2026 Bundibugyo outbreak lacks all three.
The recovery of more than 100 patients by late June 2026 demonstrates that supportive care protocols are producing results and that the health system, under extreme pressure, is still functioning. Analysing the global cobalt supply picture alongside this evolving health emergency underscores just how intertwined the humanitarian and economic dimensions of this crisis have become.
Key Metrics: The 2026 DR Congo Bundibugyo Ebola Outbreak at a Glance
| Dimension | Current Status |
|---|---|
| Causative pathogen | Bundibugyo virus (BDBV) |
| WHO emergency classification | PHEIC declared |
| DRC confirmed cases | 1,003+ |
| DRC confirmed deaths | 254+ |
| Uganda confirmed cases | 19 |
| Uganda confirmed deaths | 2 |
| Approved strain-specific vaccine | None |
| Primary affected provinces | Ituri, North Kivu, South Kivu |
| U.S. emergency funding activated | $107 million |
| Global economic exposure | Cobalt and copper supply chains |
| Outbreak trajectory | Accelerating as of late June 2026 |
Frequently Asked Questions: DR Congo Bundibugyo Ebola Outbreak
What makes the Bundibugyo strain different from other Ebola viruses?
Bundibugyo virus is a taxonomically distinct species within the Ebolavirus genus, with its own antigenic profile. This means that vaccines and therapeutic antibodies developed for Zaire ebolavirus, the strain targeted by all currently licensed Ebola vaccines, do not have confirmed efficacy against BDBV. The strain was first identified in Uganda in 2007 and has historically produced case fatality ratios between 25 and 36 percent.
How many confirmed cases and deaths have been recorded in the 2026 outbreak?
As of late June 2026, DRC has confirmed more than 1,003 cases and 254 deaths. Uganda has recorded 19 confirmed cases and 2 deaths. Health officials and WHO have indicated that the true infection count is very likely substantially higher than these confirmed figures.
Has this outbreak been declared a global health emergency?
Yes. WHO has declared the 2026 DR Congo Bundibugyo Ebola outbreak a Public Health Emergency of International Concern (PHEIC), the highest alert designation available under international health law. This triggers mandatory reporting obligations for WHO member states and activates expedited international response mechanisms.
Which provinces are most severely affected?
The outbreak is concentrated in Ituri Province in northeastern DRC, with additional confirmed cases in North Kivu and South Kivu. All three provinces sit in the conflict-affected eastern region of the country.
Why does this outbreak carry implications for global supply chains?
DRC produces approximately 70 to 75 percent of global cobalt and is a major copper producer. The provinces at the outbreak's epicentre overlap with or are adjacent to extraction zones supplying these minerals to global electric vehicle battery and clean energy supply chains. Sustained disruption to the region's workforce and logistics infrastructure carries potential consequences for global commodity markets.
Is there an approved vaccine being used to control this outbreak?
No approved vaccine exists specifically for Bundibugyo virus. Response teams are relying on isolation, contact tracing, community engagement, and supportive care. Experimental countermeasures and potential compassionate use of cross-reactive monoclonal antibody therapies are under consideration, and the WHO R&D Blueprint framework may be invoked to accelerate Bundibugyo-specific countermeasure development.
Want to Stay Ahead of Supply Chain Disruptions Affecting ASX-Listed Commodity Stocks?
The DR Congo Bundibugyo Ebola outbreak highlights just how rapidly humanitarian crises can intersect with critical minerals markets — and how quickly cobalt and copper supply chain risks can shift the investment landscape for ASX-listed resource companies. Discovery Alert's proprietary Discovery IQ model delivers real-time alerts on significant ASX mineral discoveries, helping investors identify actionable opportunities the moment they emerge — explore historic discovery returns on Discovery Alert's dedicated discoveries page and begin your 14-day free trial to stay ahead of the market.